Technologies That Shape Neural Activity
From magnetic pulses to focused ultrasound — the science of non-invasive and invasive brain stimulation, grounded in clinical research and quantitative specifications.
Historical Context of Neuromodulation
The idea of using electricity to influence the brain dates back to antiquity. Roman physician Scribonius Largus described applying electric torpedo fish to the head for headache relief in 46 AD. Modern neuromodulation began in the 1980s when Anthony Barker and colleagues at the University of Sheffield demonstrated the first successful transcranial magnetic stimulation (TMS) of the human motor cortex in 1985, producing visible hand twitches without invasive procedures.[42]
This breakthrough opened the door to non-invasive brain stimulation research. Deep Brain Stimulation (DBS) was pioneered by Alim-Louis Benabid in 1987 at the University of Grenoble, who discovered that high-frequency electrical stimulation of the ventral intermediate nucleus of the thalamus could suppress tremor in Parkinson's disease patients. The FDA approved DBS for essential tremor in 1997 and for Parkinson's disease in 2002.[1][7]
The field has since expanded dramatically: tDCS emerged in the early 2000s as a low-cost, portable alternative; tACS was developed to entrain brain oscillations at specific frequencies; and focused ultrasound neuromodulation has rapidly advanced since 2010, offering a path to non-invasive deep brain stimulation without surgery.
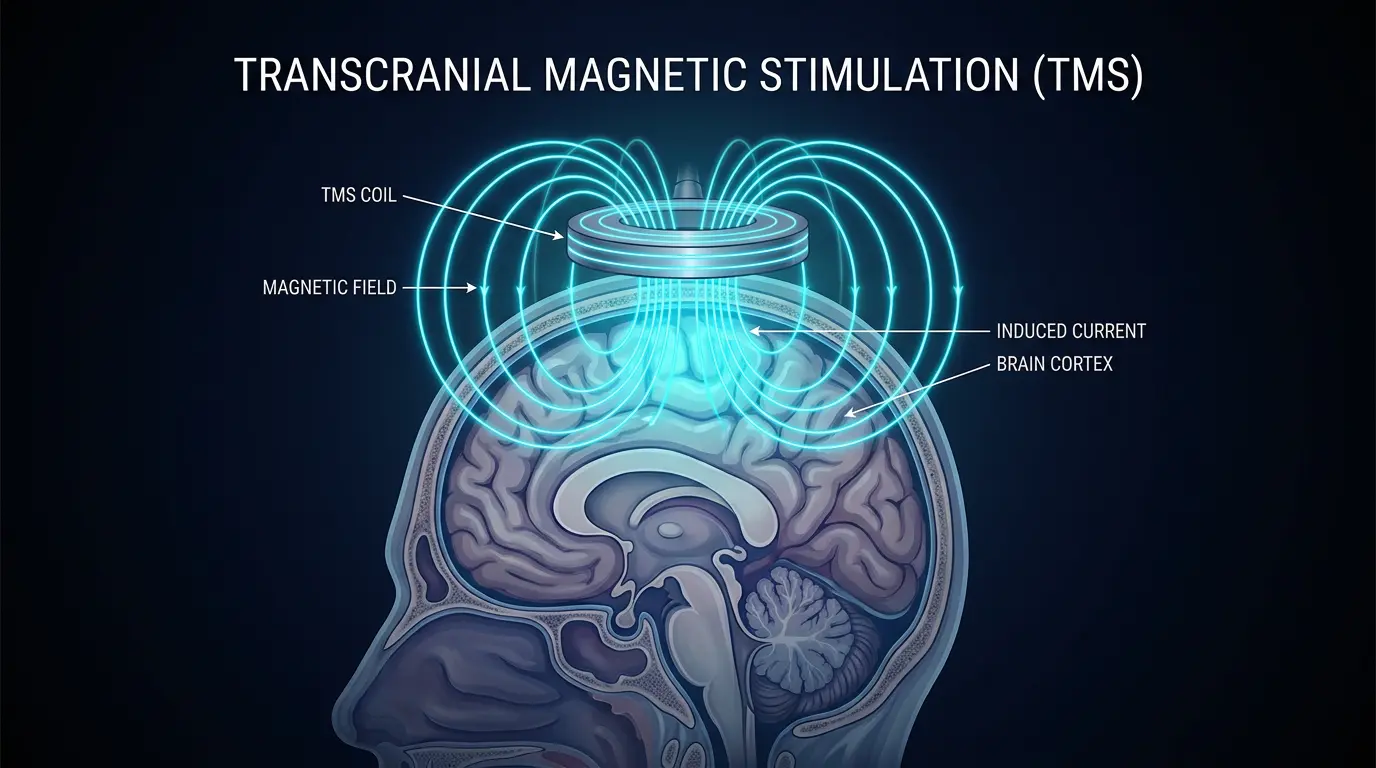
Transcranial Magnetic Stimulation (TMS)
TMS utilizes rapidly changing magnetic fields (1.5–3 Tesla at the coil surface) to induce electrical currents in superficial cortical tissue. The technique works by electromagnetic induction: a brief, high-current pulse (up to 8,000 amperes) through a copper coil generates a time-varying magnetic field that penetrates the skull with minimal attenuation and induces secondary electric currents (~100–200 mV/m) in the underlying cortex.[1][7][42]
FDA-approved for treatment-resistant depression since 2008, repetitive TMS (rTMS) has demonstrated significant efficacy across multiple neurological and psychiatric conditions. Theta-burst stimulation (TBS) protocols — delivering 600 pulses in just 3 minutes — achieve response rates for major depressive disorder comparable to weeks-long standard rTMS protocols. The Stanford Accelerated Intelligent Neuromodulation Therapy (SAINT) protocol delivers multiple daily sessions over 5 days and has shown remission rates exceeding 78% in treatment-resistant depression.[1][26][51]
Coil Geometries & Depth of Penetration
The standard figure-of-eight coil achieves focality of ~1–2 cm² at the cortical surface but is limited to superficial cortex (~2–3 cm deep). The H-coil (used in the FDA-approved Brainsway system) uses a complex multi-loop geometry to stimulate deeper structures up to ~4–6 cm, though with reduced focality. Novel coil designs including the double-cone coil can reach medial cortical structures like the cingulate cortex.[7][51]
Navigated TMS & Precision Mapping
Modern navigated TMS (nTMS) combines real-time MRI-based neuronavigation with electromyographic (EMG) monitoring, enabling precise mapping of functional cortical areas — particularly the motor and language cortices. This has become a valuable presurgical planning tool for brain tumor resections, identifying eloquent cortex with millimeter-level accuracy. nTMS motor mapping has been shown to reduce post-surgical morbidity by up to 30% compared to direct cortical stimulation alone.[43][51]
Key Specifications
Transcranial Direct Current Stimulation (tDCS)
tDCS applies weak direct currents (typically 1–2 mA) through scalp-placed electrodes to modulate neuronal excitability. The electric field produced at the cortical level is approximately 0.3–0.8 V/m, far below the threshold for direct action potential generation. Instead, tDCS shifts the resting membrane potential of neurons, altering their probability of firing in response to synaptic inputs.[7][8][52]
Effects are polarity-dependent: anodal stimulation (positive electrode over target region) depolarizes the neuronal membrane, increasing excitability by ~20–40%. Cathodal stimulation hyperpolarizes it, decreasing excitability. The after-effects can persist for 60–90 minutes following a 20-minute session, mediated by NMDA receptor-dependent long-term potentiation (LTP) and long-term depression (LTD) mechanisms.[52]
Clinical Applications & Limitations
While less focused than TMS, tDCS is significantly more portable (battery-powered, ~$500–2,000 devices) and is actively investigated for depression, chronic pain, stroke rehabilitation, and cognitive enhancement. Home-based tDCS protocols supervised remotely have shown promise for increasing treatment accessibility. However, the low spatial resolution means that current spreads across multiple brain regions, making precise targeting difficult. Computational head models using individual MRI scans are increasingly used to optimize electrode placement.[7]
Current Flow Modeling
The distribution of current through the brain during tDCS is highly non-uniform and depends on individual anatomy — skull thickness, CSF distribution, and cortical folding all influence the electric field pattern. Finite element modeling (FEM) using MRI-derived head models has revealed that peak electric fields often occur at locations distant from the electrodes, particularly at CSF-filled sulcal boundaries where current density concentrates. This has led to the development of HD-tDCS (High-Definition tDCS) using arrays of small electrodes for improved focality (~1 cm² vs. 25–35 cm²).[52]
Key Specifications
Transcranial Alternating Current Stimulation (tACS)
tACS delivers sinusoidal alternating currents through scalp electrodes at specific frequencies, aiming to entrain endogenous brain oscillations. Unlike tDCS which shifts baseline excitability, tACS targets the temporal dynamics of neural activity by synchronizing local field potentials to the applied frequency.[52][53]
The technique leverages the fact that brain function depends critically on oscillatory coordination between neural populations. Different frequency bands serve distinct functions:
Research has demonstrated that 10 Hz (alpha-band) tACS applied over the visual cortex can modulate phosphene thresholds and visual perception. Gamma-frequency tACS (40 Hz) applied to frontal cortex has shown effects on working memory performance. Multi-electrode tACS can even phase-synchronize or desynchronize activity between distant brain regions, offering a tool to study functional connectivity.[53]
Key Specifications
Deep Brain Stimulation (DBS)
DBS is the gold standard for precision neuromodulation, requiring invasive surgical implantation of electrodes directly into deep brain structures. It has demonstrated exceptional efficacy in managing Parkinson's disease, essential tremor, and dystonia by delivering targeted electrical stimulation to nuclei like the subthalamic nucleus (STN) or globus pallidus internus (GPi).[1][6]
Mechanism of Action
Despite over three decades of clinical use, the exact mechanism of DBS remains debated. The prevailing hypothesis is that high-frequency stimulation (typically 130 Hz) creates an "informational lesion" that disrupts pathological oscillatory activity in basal ganglia-thalamocortical circuits. Recent evidence suggests DBS may also release neurotransmitters (GABA, glutamate, adenosine) from stimulated neurons and modulate network-level synchronization across wide brain areas.[7][54]
Adaptive (Closed-Loop) DBS
Traditional DBS delivers constant stimulation regardless of the patient's state. Next-generation adaptive DBS (aDBS) systems use real-time biomarkers — particularly beta-band (13–30 Hz) oscillatory power in the STN — to modulate stimulation intensity dynamically. Clinical trials have shown aDBS reduces stimulation time by ~50% while maintaining or improving motor outcomes, with fewer side effects such as dysarthria and gait disturbance.[54]
Expanding Clinical Indications
Beyond movement disorders, DBS is being actively investigated for treatment-resistant depression (targeting the subcallosal cingulate, Brodmann Area 25), obsessive-compulsive disorder (ventral capsule/ ventral striatum), epilepsy (anterior nucleus of the thalamus — FDA-approved via the SANTE trial), Alzheimer's disease (fornix stimulation), and addiction (nucleus accumbens).[1][54]
Key Specifications
Transcranial Focused Ultrasound (TUS)
Focused ultrasound is rapidly emerging as the most promising non-invasive neuromodulation technique, combining depth and precision that neither TMS nor tDCS can achieve. TUS uses acoustic energy in the sub-MHz frequency range (typically 250 kHz – 1 MHz) that passes through the skull and can be focused on a target as small as a 1 mm sphere deep within the brain.[6][7][19]
Mechanisms: Thermal vs. Mechanical
TUS operates through two primary mechanisms depending on intensity. At low intensities (ISPTA < 720 mW/cm²), the primary effect is mechanical — acoustic radiation force and microcavitation create pressure fluctuations that modulate mechanosensitive ion channels (TREK-1, TRAAK, Piezo1) in neuronal membranes. At high intensities (ISPTA > 1 W/cm²), thermal ablation is the primary mechanism, used clinically in MRI-guided focused ultrasound (MRgFUS) for essential tremor treatment via thalamotomy.[6][13][20]
Landmark Clinical Achievements
A landmark 2025 study by Darmani et al. published in Nature Communications demonstrated individualized stimulation of the basal ganglia using low-intensity TUS, validating its potential as a non-invasive DBS alternative. Target engagement was confirmed in patients with existing DBS leads, showing precise modulation of the globus pallidus internus. The study used patient-specific acoustic simulations based on CT skull data to correct for phase aberrations caused by the irregular skull bone.[1][6][19]
Additionally, the first randomized controlled trial of TUS for depression (targeting the right frontal pole) published in 2024 showed significant improvement in MADRS depression scores compared to sham stimulation, with effects persisting for 4 weeks post-treatment.[20][24]
Key Specifications
Safety Profiles & Dosimetry
All neuromodulation techniques carry risk-benefit profiles that vary significantly by modality. Comprehensive safety frameworks have been established by international consensus panels including the IFCN (International Federation of Clinical Neurophysiology) and the ITRUSST (International Transcranial Ultrasonic Stimulation Safety and Standards).[7][43]
| Modality | Common Side Effects | Serious Risks | Seizure Risk |
|---|---|---|---|
| TMS | Scalp discomfort, headache, muscle twitching | Seizure (rare: <0.01%) | ~1:30,000 |
| tDCS | Tingling, itching, mild redness under electrodes | Skin burns (poor contact), phosphenes | Extremely rare |
| DBS | Dysarthria, paresthesia, mood changes | Hemorrhage (1–2%), infection (3–5%) | <1% |
| TUS | Transient auditory percept, mild headache | None reported at diagnostic levels | None reported |
Dosimetry Considerations
Dosimetry in neuromodulation remains an active challenge. Unlike pharmacology where a "dose" has a clear definition, neuromodulation dose depends on multiple interacting parameters: intensity, frequency, duration, electrode/coil geometry, individual anatomy, and brain state at the time of stimulation. Computational modeling is increasingly used to estimate the electric field distribution in individual brains, but standardized dose reporting remains elusive. The IFCN has published guidelines for minimum reporting standards.[43][7]
Technology Comparison Matrix
Comparative scoring (0–10) across invasiveness, depth of penetration, spatial precision, and field strength for six key neuromodulation and BCI technologies.