Electromagnetic Control of Motor Functions
How TMS, functional electrical stimulation, epidural spinal stimulation, and brain-computer interfaces can trigger, restore, or override human motor activity — a research-backed analysis of demonstrated capabilities and physical limits.
Transcranial Magnetic Stimulation — Motor Cortex Excitation
Transcranial magnetic stimulation (TMS) was first demonstrated by Barker, Jalinous & Freeston in 1985, showing that a brief, intense magnetic pulse applied over the motor cortex could induce involuntary muscle contractions in the contralateral hand — the first non-invasive, painless demonstration of electromagnetic control over the human motor system.[42]
Single-pulse TMS over the primary motor cortex (M1) generates a motor evoked potential (MEP) — a measurable electrical response in the target muscle, typically recorded via electromyography (EMG) in the hand muscles (first dorsal interosseous or abductor pollicis brevis). The latency from cortical stimulation to peripheral muscle activation is approximately 20–25 ms for hand muscles, reflecting corticospinal conduction through the pyramidal tract.[43]
Motor Evoked Potentials (MEPs)
MEPs are the gold-standard readout of corticomotor excitability. A single TMS pulse at ~120% of motor threshold (typically 40–60% of maximum stimulator output) generates reproducible muscle twitches. The amplitude, latency, and threshold of MEPs allow researchers to map the motor cortex, assess spinal cord integrity, and diagnose conditions such as multiple sclerosis or amyotrophic lateral sclerosis (ALS).[42][43]
Repetitive TMS (rTMS) — Lasting Motor Effects
Repetitive TMS delivered at specific frequencies can produce effects that outlast the stimulation period. High-frequency rTMS (≥5 Hz) over M1 increases cortical excitability and MEP amplitudes for 15–30 minutes after stimulation. Low-frequency rTMS (≤1 Hz) suppresses excitability. These protocols form the basis of therapeutic rTMS for stroke rehabilitation and chronic pain.[43]
Cortical Mapping
By systematically moving the TMS coil across the scalp and recording MEPs from different muscles, researchers can construct detailed maps of the motor cortex — determining the precise cortical representation of hand, arm, face, and leg muscles. This non-invasive mapping technique confirms the classic Penfield homunculus and reveals individual variations in motor cortex organization.[42]
Key Insight: TMS demonstrates that a single magnetic pulse, delivered at the correct location and intensity, can activate the entire motor output chain — from cortex to spinal cord to peripheral muscle — producing a measurable, involuntary contraction. The coil must be within 1–3 cm of the scalp.
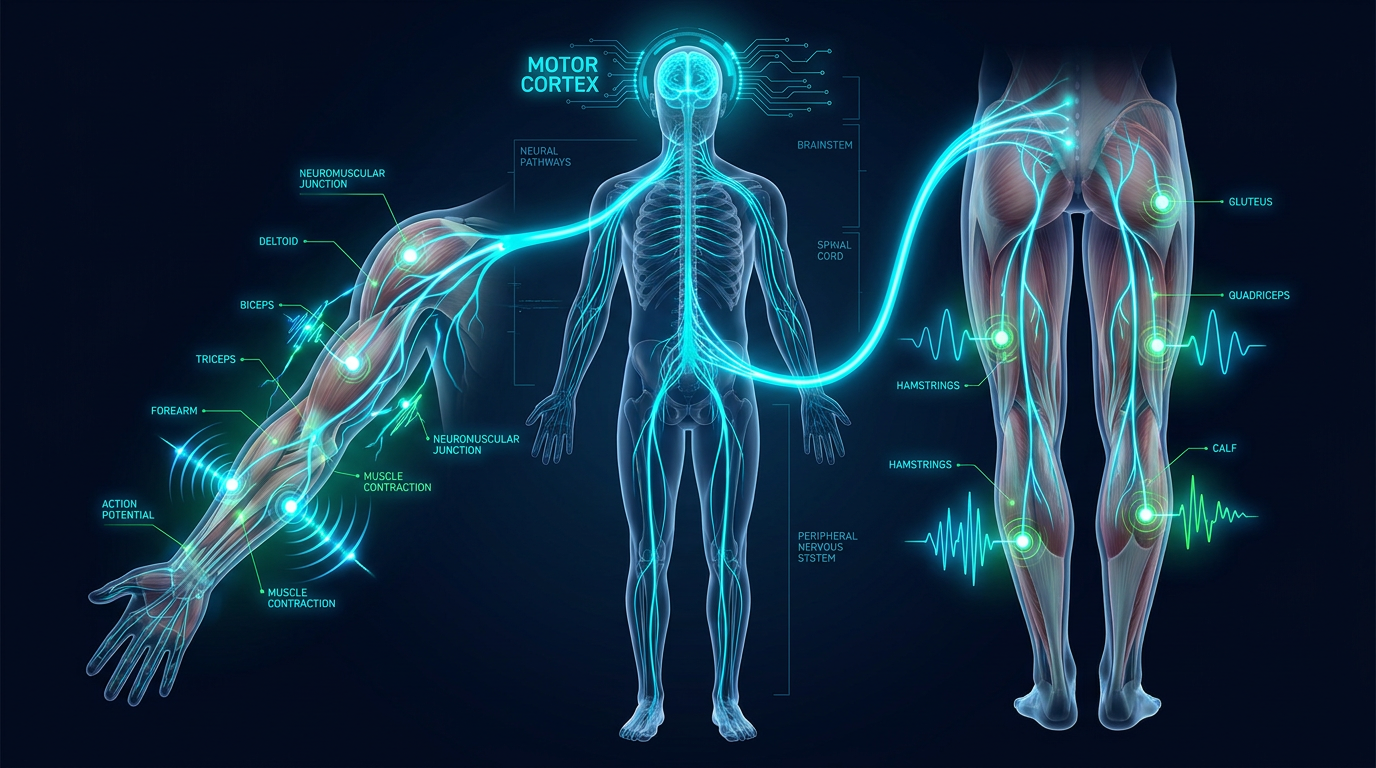
Motor Control Pathway — From Cortex to Muscle
Motor pathway from primary motor cortex (M1) through corticospinal tract, spinal cord, and neuromuscular junction to skeletal muscle. Intervention points shown for TMS, epidural stimulation, FES, and BCI recording.
Functional Electrical Stimulation — Peripheral Motor Restoration
Functional Electrical Stimulation (FES) bypasses the brain entirely, delivering electrical current directly to motor nerves or muscles through surface or implanted electrodes. FES has been used clinically since the 1960s to restore functional movement in paralyzed limbs — enabling hand grasp in tetraplegic patients, standing in paraplegic patients, and foot-drop correction during gait.[44]
Modern FES systems use multi-channel electrode arrays with sophisticated pulse patterns. Typical stimulation parameters include biphasic pulses at 20–50 Hz, with pulse widths of 200–500 μs and current amplitudes of 20–100 mA. The electrical parameters must be carefully tuned to produce smooth, functional movements without fatigue or pain.[44]
FES for Hand Grasp
Surface FES applied to the forearm muscles (flexor digitorum superficialis and extensor digitorum communis) can produce coordinated hand opening and closing. Systems like the Freehand device used implanted electrodes to give C5/C6 tetraplegic patients functional grasp and release — controlled by contralateral shoulder movement.[44]
FES Cycling & Locomotion
Multi-channel FES can activate quadriceps, hamstrings, and gluteal muscles in a coordinated sequence to produce pedaling motion on a stationary ergometer. FES-assisted cycling has been used therapeutically to maintain muscle mass, improve cardiovascular fitness, and enhance bone density in spinal cord injury patients.[44]
Critical Distinction: FES requires direct electrical contact with the target tissue — either through skin-surface electrodes or surgically implanted leads. Typical electrode-to-nerve distances are 0–5 mm. This is fundamentally incompatible with any remote or space-based stimulation concept.
Epidural Spinal Cord Stimulation — Restoring Locomotion
In a series of landmark studies, Grégoire Courtine and colleagues at EPFL demonstrated that epidural electrical stimulation (EES) of the lumbosacral spinal cord can restore standing and walking in individuals with chronic complete spinal cord injury. The key insight: the spinal cord contains intrinsic locomotor circuits (central pattern generators) that can be reactivated by targeted electrical stimulation, even years after injury.[45]
The STIMO (Stimulation Movement Overground) clinical trial demonstrated that three participants with chronic complete paraplegia recovered voluntary control of previously paralyzed leg muscles after several months of rehabilitation combined with spatiotemporal EES. The stimulation used a 16-electrode paddle array placed over the posterior roots of L1–S2, with electrode configurations targeting specific motor pools to enable flexion and extension in a walking pattern.[45][46]
Spatiotemporal Stimulation
Unlike continuous stimulation, EES for locomotion uses spatiotemporally patterned sequences: different electrode combinations activate different motor pools in a timed pattern that mimics the natural firing sequence during walking. This requires precise real-time control with stimulation parameters updated every 20–40 ms, synchronized with the gait cycle via inertial measurement units.[45]
Brain-Spine Interface (BSI)
In 2023, Lorach et al. published a brain-spine interface that wirelessly linked cortical recording electrodes (over the motor cortex) to the epidural spinal stimulator. This allowed a paralyzed individual to control his own leg movements via thought — the cortical signals were decoded in real time and converted to spinal stimulation commands, restoring relatively natural walking.[46]
Neuroplasticity & Recovery
Remarkably, prolonged EES rehabilitation led to neuroplastic changes: some participants eventually recovered voluntary leg movement even without stimulation. This suggests that EES reactivates dormant neural pathways and promotes axonal sprouting across the lesion site, enabling genuine neural recovery.[45][46]
Key Finding: Epidural stimulation demonstrates that the spinal cord itself is a programmable motor controller. However, the electrodes must be surgically implanted within ~1 mm of the dorsal rootlets. Even 2–3 mm displacement dramatically reduces specificity and effectiveness.
BCI-Driven Motor Prosthetics — Thought-Controlled Movement
Brain-computer interfaces represent the most sophisticated form of electromagnetic motor control: recording neural activity from the motor cortex and decoding movement intentions to drive external actuators — robotic arms, computer cursors, or the patient's own muscles via FES.[47]
The BrainGate consortium has led intracortical BCI development since the early 2000s. Using the Utah Array — a 96-channel microelectrode array (4×4 mm) implanted in the hand area of M1 — tetraplegic participants have demonstrated cursor control on a computer, robotic arm operation to grasp and drink from a bottle, and even FES-mediated restoration of hand grasp in their own paralyzed limb.[47][3]
Intracortical Somatosensory Feedback
Flesher et al. (2021) achieved a major milestone: adding somatosensory feedback to a BCI motor prosthetic. By delivering intracortical microstimulation (ICMS) to the somatosensory cortex synchronized with robotic finger contact, a tetraplegic participant could feel what the robotic hand was touching — doubling the speed of object manipulation compared to visual-only feedback.[47]
Decoding Accuracy
Modern intracortical BCIs achieve remarkable decoding accuracy: 95% or better for 2D cursor control, 90%+ for robotic arm reach-and-grasp tasks, and real-time typing speeds of 90+ characters per minute (Stanford, 2021). These systems demonstrate that motor intentions can be read from neural populations of just 100–200 neurons with sufficient precision for functional control.[3][47]
Non-Invasive BCI Limitations
EEG-based BCIs (non-invasive) can achieve basic motor intent classification — left vs. right hand movement imagination — but with far lower bandwidth (information transfer rates of 10–25 bits/min vs. hundreds for intracortical BCIs). The skull and scalp attenuate and blur neural signals by a factor of ~10,000, fundamentally limiting spatial resolution.[2]
Key Insight: Even the most advanced BCIs require electrodes implanted into the brain to achieve high-bandwidth motor control. Non-invasive approaches offer orders-of-magnitude less precision. Reading motor intent from orbit is physically impossible with any known or theoretically foreseeable technology.
Implications & Physical Constraints
All four demonstrated techniques for electromagnetic motor control share a common requirement: extreme proximity between the stimulation source and the target neural tissue. TMS coils must be within 1–3 cm of the cortex. FES electrodes contact the skin or are implanted in muscle. Epidural stimulators sit within 1 mm of spinal roots. BCI arrays are inserted directly into brain tissue.
Proximity Is Non-Negotiable
The magnetic field from a TMS coil drops as 1/r³. Doubling the distance reduces the induced electric field 8-fold. At satellite altitude (~550 km), the field is effectively zero.
Specificity Requires Contact
FES and epidural stimulation achieve motor specificity because electrodes target individual nerve roots or muscles. Broad-field stimulation from distance would activate everything simultaneously — producing seizures, not coordinated movement.
Reading ≠ Writing
BCI motor control requires both reading (recording neural signals) and writing (delivering feedback stimulation). Each direction faces separate, compounding physical barriers at distance.
The 10¹⁷ Power Gap
The most optimistic satellite power density at ground (~10⁻⁸ W/m²) is 17 orders of magnitude below the weakest known neural activation threshold. No antenna gain or orbital maneuver closes this gap.